
Movilización pasiva continua en pacientes con artroplastia de rodilla
Resumen
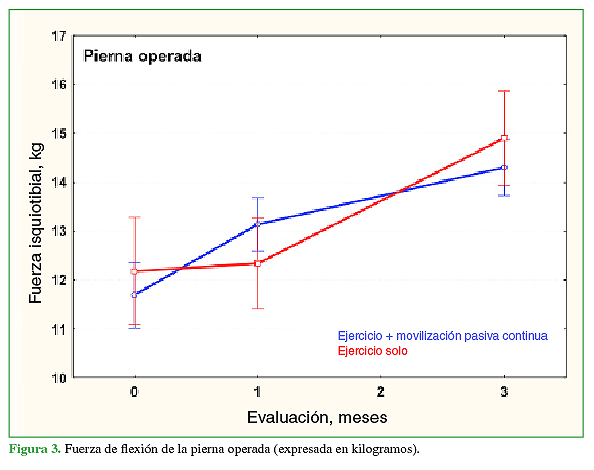
Introducción: La artroplastia total de rodilla es el recurso terapéutico para pacientes con artrosis severa y gran incapacidad física. Sin embargo, muchos evolucionan con dolor y déficit funcional. En este estudio, se utiliza un tratamiento con movilización pasiva continua a partir de los 10 días de la cirugía. Materiales y Métodos: Se incluyó a 60 pacientes que fueron asignados, en forma aleatoria, a 2 grupos (30 en cada grupo). Al grupo 1 (G1, 23 mujeres) se le aplicó un protocolo de tratamiento convencional y, al grupo 2 (G2, 17 mujeres), el mismo programa y la adicción de un equipo de movimiento pasivo continuo a los 10 días de la intervención. Se evaluaron el dolor, la movilidad articular, la fuerza muscular y la función (WOMAC y prueba TUG). Resultados: No se observaron diferencias estadísticamente significativas en los parámetros estudiados, aunque sí una tendencia a la mejoría en el G2. En este grupo, la fuerza de extensión de la rodilla fue mayor y también hubo una correlación basal entre la fuerza y la prueba TUG. Conclusiones: El uso diferido de la movilización pasiva continua mejoró la fuerza de extensión de la rodilla y el rendimiento en la prueba TUG, aunque sin diferencias significativas entre ambos grupos. No se observaron efectos adversos. Nivel de Evidencia: IDescargas
Citas
Tang X, Wang S, Zhan S, Niu J, Tao K, Zhang Y, et al. The prevalence of symptomatic knee osteoarthritis in China: results from the China Health and Retirement Longitudinal Study. Arthritis Rheumatol 2016;68(3):648-53.
https://doi.org/10.1002/art.39465
Plotnikoff R, Karunamuni N, Lytvyak E, Penfold C, Schopflocher D, Imayama I, et al. Osteoarthritis prevalence and modifiable factors: a population study. BMC Public Health 2015;15:1195. https://doi.org/10.1186/s12889-015-2529-0
Dillon CF, Rasch EK, Gu Q, Hirsch R. Prevalence of knee osteoarthritis in the United States: arthritis data
from the Third National Health and Nutrition Examination Survey 1991-94. J Rheumatol 2006;33(11):2271-9.
PMID: 17013996
Turkiewicz A, Gerhardsson de Verdier M, Engström G, Nilsson PM, Mellström C, Lohmander LS, et al. Prevalence of knee pain and knee OA in southern Sweden and the proportion that seeks medical care. Rheumatology (Oxford) 2015;54(5):827-35. https://doi.org/10.1093/rheumatology/keu409
Castell MV, van der Pas S, Otero A, Siviero P, Dennison E, Denkinger M, et al. Osteoarthritis and frailty in elderly individuals across six European countries: results from the European Project on OSteoArthritis (EPOSA). BMC Musculoskelet Disord 2015;16:359. https://doi.org/10.1186/s12891-015-0807-8
National Institutes of Health Consensus Program. NIH Consensus Development Conference on Total Knee
Replacement – Final Statement. Disponible en: https://consensus.nih.gov/2003/2003totalkneereplacement117html.htm
Lizaur A, Marco L, Cebrian R. Preoperative factors influencing the range of movement after total knee arthroplasty for severe osteoarthritis. J Bone Joint Surg Br 1997;79(4):626-9. https://doi.org/10.1302/0301-620x.79b4.7242
Farahini H, Moghtadaei M, Bagheri A, Akbarian E. Factors influencing range of motion after total knee arthroplasty. Iran Red Crescent Med J 2012;14(7):417-21. PMID: 22997557
Naili JE, Iversen MD, Esbjörnsson AC, Hedström M, Schwartz MH, Häger CK, et al. Deficits in functional
performance and gait one year after total knee arthroplasty despite improved self-reported function. Knee Surg
Sports Traumatol Arthrosc 2017;25(11):3378-86. https://doi.org/10.1007/s00167-016-4234-7
Mizner RL, Petterson SC, Clements KE, Zeni JA Jr, Irrgang JJ, Snyder-Mackler L. Measuring functional
improvement after total knee arthroplasty requires both performance-based and patient-report assessments: a
longitudinal analysis of outcomes. J Arthroplasty 2011;26(5):728-37. https://doi.org/10.1016/j.arth.2010.06.004
Bade MJ, Kohrt WM, Stevens-Lapsley JE. Outcomes before and after total knee arthroplasty compared to healthy adults. J Orthop Sports Phys Ther 2010;40(9):559-67. https://doi.org/10.2519/jospt.2010.3317
Ransen M, Nairn L, Bridgett L, Crosbie J, March L, Parker D, et al. Post-acute rehabilitation after total knee
replacement: a multicenter randomized clinical trial comparing long-term outcomes. Arthritis Care Res
;69:192-200. https://doi.org/10.1002/acr.23117
Ishii Y, Noguchi H, Sato J, Sakurai T, Toyabe SI. Quadriceps strength impairment in the mid- to long-term followup period after total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc 2017;25(11):3372-7.
https://doi.org/10.1007/s00167-016-4333-5
Kievit AJ, van Geenen RC, Kuijer PP, Pahlplatz TM, Blankevoort L, Schafroth MU. Total knee arthroplasty and the unforeseen impact on return to work: a cross-sectional multicenter survey. J Arthroplasty 2014;29(6):1163-8.
https://doi.org/10.1016/j.arth.2014.01.004
Postel JM, Thoumie P, Missaoui B, Biau D, Ribinik P, Revel M, Rannou F; French Physical Medicine and
Rehabilitation Society. Continuous passive motion compared with intermittent mobilization after total knee
arthroplasty. Elaboration of French clinical practice guidelines. Ann Readapt Med Phys 2007;50(4):244-57.
https://doi.org/10.1016/j.annrmp.2007.03.001
O’Driscoll SW, Giori NJ. Continuous passive motion (CPM): theory and principles of clinical application. J Rehabil Res Dev 2000;37(2):179-88. PMID: 10850824
Harvey LA, Brosseau L, Herbert RD. Continuous passive motion following total knee arthroplasty in people with arthritis. Cochrane Database Syst Rev 2010;(2):CD004260. https://doi.org/10.1002/14651858.CD004260.pub3
Brosseau L, Milne S, Wells G, Tugwell P, Robinson V, Casimiro L, et al. Efficacy of continuous passive motion
following total knee arthroplasty: a metaanalysis. J Rheumatol 2004;31(11):2251-64. PMID: 15517640
Maniar RN, Baviskar JV, Singhi T, Rathi SS. To use or not to use continuous passive motion post-total knee
arthroplasty presenting functional assessment results in early recovery. J Arthroplasty 2012;27(2):193-200.e1.
https://doi.org/10.1016/j.arth.2011.04.009
Alkire MR, Swank ML. Use of inpatient continuous passive motion versus no CPM in computer-assisted total knee arthroplasty. Orthop Nurs 2010;29(1):36-40. https://doi.org/10.1097/NOR.0b013e3181c8ce23
Lenssen AF, Crijns YH, Waltjé EM, Roox GM, van Steyn MJ, Geesink RJ, et al. Effectiveness of prolonged use
of continuous passive motion (CPM) as an adjunct to physiotherapy following total knee arthroplasty: design of a
randomised controlled trial [ISRCTN85759656]. BMC Musculoskelet Disord 2006;7:15.
https://doi.org/10.1186/1471-2474-7-15
Bruun-Olsen V, Heiberg KE, Mengshoel AM. Continuous passive motion as an adjunct to active exercises in early rehabilitation following total knee arthroplasty - a randomized controlled trial. Disabil Rehabil 2009;31(4):277-83. https://doi.org/10.1080/09638280801931204
Denis M, Moffet H, Caron F, Ouellet D, Paquet J, Nolet L. Effectiveness of continuous passive motion and
conventional physical therapy after total knee arthroplasty: a randomized clinical trial. Phys Ther 2006;86(2):174-
PMID: 16445331
Joshi RN, White PB, Murray-Weir M, Alexiades MM, Sculco TP, Ranawat AS. Prospective randomized trial of the
efficacy of continuous passive motion post total knee arthroplasty: experience of the Hospital for Special Surgery. J Arthroplasty 2015;30(12):2364-9. https://doi.org/10.1016/j.arth.2015.06.006
Chen LH, Chen CH, Lin SY, Chien SH, Su JY, Huang CY, et al. Aggressive continuous passive motion exercise
does not improve knee range of motion after total knee arthroplasty. J Clin Nurs 2013;22(3-4):389-94.
https://doi.org/10.1111/j.1365-2702.2012.04106.x
Boese CK, Weis M, Phillips T, Lawton-Peters S, Gallo T, Centeno L. The efficacy of continuous passive motion
after total knee arthroplasty: a comparison of three protocols. J Arthroplasty 2014;29(6):1158-62.
https://doi.org/10.1016/j.arth.2013.12.005
Worland RL, Arredondo J, Angles F, Lopez-Jimenez F, Jessup DE. Home continuous passive motion machine
versus professional physical therapy following total knee replacement. J Arthroplasty 1998;13(7):784-7.
https://doi.org/10.1016/s0883-5403(98)90031-6
Lotke PA, Faralli VJ, Orenstein EM, Ecker ML. Blood loss after total knee replacement. Effects of tourniquet
release and continuous passive motion. J Bone Joint Surg Am 1991;73(7):1037-40. PMID: 1874765
Pope RO, Corcoran S, McCaul K, Howie DW. Continuous passive motion after primary total knee arthroplasty.
Does it offer any benefits? J Bone Joint Surg Br 1997;79(6):914-7. https://doi.org/10.1302/0301-620x.79b6.7516
Pua YH1, Ong PH, Chong HC, Yeo W, Tan C, Lo NN. Knee extension range of motion and self-report physical
function in total knee arthroplasty: mediating effects of knee extensor strength. BMC Musculoskelet Disord
;14:33. https://doi.org/10.1186/1471-2474-14-33
Holm B, Kristensen MT, Bencke J, Husted H, Kehlet H, Bandholm T. Loss of knee-extension strength is related to knee swelling after total knee arthroplasty. Arch Phys Med Rehabil 2010;91(11):1770-6.
https://doi.org/10.1016/j.apmr.2010.07.229
Escobar A, Quintana JM, Bilbao A, Azkárate J, Güenaga JI. Validation of the Spanish version of the WOMAC
questionnaire for patients with hip or knee osteoarthritis. Western Ontario and McMaster Universities Osteoarthritis Index. Clin Rheumatol 2002;21(6):466-71. https://doi.org/10.1007/s100670200117
Podsiadlo D, Richardson S. The timed “Up & Go”: a test of basic functional mobility for frail elderly persons.
J Am Geriatr Soc 1991;39(2):142-8. https://doi.org/10.1111/j.1532-5415.1991.tb01616.x
Suri S, Gill SE, Massena de Camin S, Wilson D, McWilliams DF, Walsh DA. Neurovascular invasion at the
osteochondral junction and in osteophytes in osteoarthritis. Ann Rheum Dis 2007;66(11):1423-8.
https://doi.org/10.1136/ard.2006.063354
Goldring SR, Goldring MB. Changes in the osteochondral unit during osteoarthritis: structure, function and
cartilage-bone crosstalk. Nat Rev Rheumatol 2016;12(11):632-44. https://doi.org/10.1038/nrrheum.2016.148
Stevens-Lapsley JE, Balter JE, Wolfe P, Eckhoff DG, Kohrt WM. Early neuromuscular electrical stimulation
to improve quadriceps muscle strength after total knee arthroplasty: a randomized controlled trial. Phys Ther
;92(2):210-26. https://doi.org/10.2522/ptj.20110124
Petterson SC, Mizner RL, Stevens JE, Raisis L, Bodenstab A, Newcomb W, et al. Improved function from
progressive strengthening interventions after total knee arthroplasty: a randomized clinical trial with an imbedded prospective cohort. Arthritis Rheum 2009;61(2):174-83. https://doi.org/10.1002/art.24167
Bade MJ, Kittelson JM, Kohrt WM, Stevens-Lapsley JE. Predicting functional performance and range of motion
outcomes after total knee arthroplasty. Am J Phys Med Rehabil 2014;93(7):579-85.
https://doi.org/10.1097/PHM.0000000000000065
Palmieri-Smith RM, Villwock M, Downie B, Hecht G, Zernicke R. Pain and effusion and quadriceps activation and strength. J Athl Train 2013;48(2):186-91. https://doi.org/10.4085/1062-6050-48.2.10
Pietrosimone BG, Hertel J, Ingersoll CD, Hart JM, Saliba SA. Voluntary quadriceps activation deficits in patients
with tibiofemoral osteoarthritis: a meta-analysis. PM R 2011;3(2):153-62; quiz 162.
https://doi.org/10.1016/j.pmrj.2010.07.485
Rice DA, McNair PJ. Quadriceps arthrogenic muscle inhibition: neural mechanisms and treatment perspectives. Semin Arthritis Rheum 2010;40(3):250-66. https://doi.org/10.1016/j.semarthrit.2009.10.001
Herbold JA, Bonistall K, Blackburn M, Agolli J, Gaston S, Gross C, et al. Randomized controlled trial of the
effectiveness of continuous passive motion after total knee replacement. Arch Phys Med Rehabil 2014;95(7):1240-5. https://doi.org/10.1016/j.apmr.2014.03.012
La aceptación del manuscrito por parte de la revista implica la no presentación simultánea a otras revistas u órganos editoriales. La RAAOT se encuentra bajo la licencia Creative Commons 4.0. Atribución-NoComercial-CompartirIgual (http://creativecommons.org/licenses/by-nc-sa/4.0/deed.es). Se puede compartir, copiar, distribuir, alterar, transformar, generar una obra derivada, ejecutar y comunicar públicamente la obra, siempre que: a) se cite la autoría y la fuente original de su publicación (revista, editorial y URL de la obra); b) no se usen para fines comerciales; c) se mantengan los mismos términos de la licencia.
En caso de que el manuscrito sea aprobado para su próxima publicación, los autores conservan los derechos de autor y cederán a la revista los derechos de la publicación, edición, reproducción, distribución, exhibición y comunicación a nivel nacional e internacional en las diferentes bases de datos, repositorios y portales.
Se deja constancia que el referido artículo es inédito y que no está en espera de impresión en alguna otra publicación nacional o extranjera.
Por la presente, acepta/n las modificaciones que sean necesarias, sugeridas en la revisión por los pares (referato), para adaptar el trabajo al estilo y modalidad de publicación de la Revista.

















