
Medial transphyseal screw placement for spastic hip treatment in children with cerebral palsy. Effectiveness and safety
Abstract
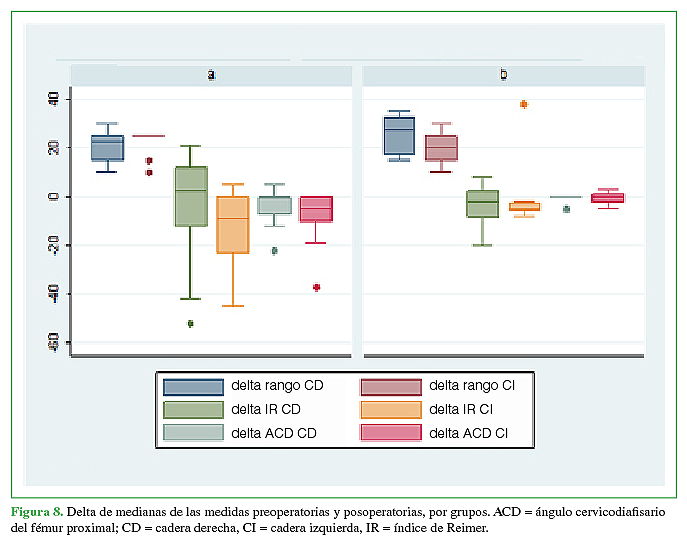
Introduction: Animal and clinical studies have shown promising results for the varus-producing placement of a medial eccentric transphyseal screw. The purpose of this study was to establish if the placement of a screw in the proximal femur is an effective and safe approach for spastic hips in children with cerebral palsy (CP). Materials and Methods: We compared two groups of pediatric CP patients (Gross Motor Function Classification System [GMFCS] III, IV and V) with “hips at risk.” Group A patients were treated with soft-tissue release plus a medial eccentric transphyseal screw in the proximal femur. Group B patients were only treated with soft-tissue release. Patients were evaluated pre- and postoperatively to determine their Rang test score, Reimer’s migration percentage (MP), neck-shaft angle (NSA), and complications. Results: From a total of 18 patients operated, 36 hips 55% (10) belonged to Group A and 45% (8) to the Group B. The median age was 51 months (IQR, 41-108). The median follow-up was 3 years (IQR, 2.4-5.8). The comparative analysis of all preoperative and postoperative variables yield only one statistically significant difference: the median left hip NSA (-5 vs. 0, P 0.02). Conclusions: The release of soft tissues was effective to prevent the spastic hip dislocation. The placement of medial eccentric transphyseal screw in spastic hips produced some complications and no beneficial changes. Medial hemiphysiodesis of the hip remains nothing but an attractive theoretical solution for the treatment of problems caused by excessive valgus. However, further studies are warranted. Level of Evidence: IIIDownloads
References
Access Economics Pty Ltd. The economic impact of cerebral palsy in Australia in 2007. Report. Australia: Cerebral Palsy Australia 2008. https://cpaustralia.com.au/media/20379/access_economics_report.pdf
Mandaleson A, Lee Y, Kerr C, Graham HK. Classifying cerebral palsy: are we nearly there? J Pediatr Orthop
;35(2):162-6. https://doi.org/10.1097/BPO.0000000000000222
Cooke PH, Cole WG, Carey RP. Dislocation of the hip in cerebral palsy. Natural history and predictability. J Bone
Joint Surg Br 1989;71(3):441-6. PMID: 2722938
Miller F, Cardoso Dias R, Dabney KW, Lipton GE, Triana M. Soft-tissue release for spastic hip subluxation in
cerebral palsy. J Pediatr Orthop 1997;17(5):571-84. https://doi.org/10.1097/00004694-199709000-00003
Flynn JM, Millar F. Management in hip disorders in patients with cerebral palsy. J Am Acad Orthop Surg
;10(3):198-209. https://doi.org/10.5435/00124635-200205000-00006
Andrisano A, Marchiodi L, Preitano M. Epiphyseodesis of the great trochanter. Ital J Orthop Traumatol
;12(2):217-22. PMID: 3793460
Davids JR, Valadie AL, Ferguson RL, Bray EW 3rd, Allen BL Jr. Surgical management of ankle valgus in children:
use of a transphyseal medial malleolar screw. J Pediatr Orthop 1997;17(1):3-8. PMID: 8989691
Stevens PM, Belle RM. Screw epiphysiodesis for ankle valgus. J Pediatr Orthop 1997;17(1):9-12. PMID: 8989692
Métaizeau JP, Wong-Chung J, Bertrand H, Pasquier P. Percutaneous epiphysiodesis using transphyseal screws
(PETS). J Pediatr Orthop 1998;18(3):363-9. PMID: 9600565
Beals RK, Shea M. Correlation of chronological age and bone age with the correction of ankle valgus by surface epiphysiodesis of the distal medial tibial physis. J Pediatr Orthop B 2005;14(6):436-8.
https://doi.org/10.1097/01202412-200511000-00009
Stevens PM, Novais EN. Multilevel guided growth for hip and knee varus secondary to chondrodysplasia. J Pediatr Orthop 2012;32(6):626-30. https://doi.org/10.1097/BPO.0b013e3182567a79
McCarthy JJ, Noonan KJ, Nemke B, Markel M. Guided growth of the proximal femur: a pilot study in the lamb
model. J Pediatr Orthop 2010;30(7):690-4. https://doi.org/10.1097/BPO.0b013e3181edef71
d’Heurle A, McCarthy J, Klimaski D, Stringer K. Proximal femoral growth modification: effect of screw, plate, and drill on asymmetric growth of the hip. J Pediatr Orthop 2018;38(2):100-4. https://doi.org/10.1097/BPO.0000000000000771
Wei-Chun Lee, Hsuan-Kai Kao, Wen-E Yang, Pei-Chi Ho, Chia-Hsieh Chang. Guided growth of the proximal femur for hip displacement in children with cerebral palsy. J Pediatr Orthop 2016;36(5):511-5.
https://doi.org/10.1097/BPO.0000000000000480
Torode IP, Young JL. Caput valgum associated with developmental dysplasia of the hip: management by
transphyseal screw fixation. J Child Orthop 2015;9(5):371-9. https://doi.org/10.1007/s11832-015-0681-9
Portinaro N, Panou A, Gagliano N, Pelillo F. D.D.S.H.: Developmental dysplasia of the spactic hip: Strategies of
management in cerebral palsy. A new suggestive algorithm. Hip Int 2009;19(Suppl 6):S69-74.
https://doi.org/10.1177/112070000901906s12
Portinaro N, Turati M, Cometto M, Bigoni M, Davids JR, Panou A. Guided growth of the proximal femur for the
management of hip dysplasia in children with cerebral palsy. J Pediatr Orthop 2019;39(8):e622-8.
https://doi.org/10.1097/BPO.0000000000001069
Carreño-Mora F, Ortiz-Corredor F, Espinosa-García E, Pérez-Hernández CE. Validación de un instrumento para
evaluar la carga del cuidador en parálisis cerebral. Rev Salud Pública (Bogota) 2015;17(4):578-88.
https://doi.org/10.15446/rsap.v17n4.35593
Dindo D, Demartines N, Clavien PA. Classification of surgical complications. A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 2004;240(2):205-13.
https://doi.org/10.1097/01.sla.0000133083.54934.ae
Presedo A, Oh CW, Dabney KW, Miller F. Soft-tissue releases to treat spastic hip subluxation in children with
cerebral palsy. J Bone Joint Surg Am 2005;87(4):832-41. https://doi.org/10.2106/JBJS.C.01099
García Mata S, Duart Clemente J. Cirugía preventiva de la luxación de cadera espástica. En: Martínez Caballero
I, Abad Lara JA (eds.). Parálisis cerebral infantil. Manejo de las alteraciones músculo-esqueléticas asociadas.
Madrid: Ergon; 2016:79-92.
Manuscript acceptance by the Journal implies the simultaneous non-submission to any other journal or publishing house. The RAAOT is under the Licencia Creative Commnos Atribución-NoComercial-Compartir Obras Derivadas Igual 4.0 Internacional (CC-BY-NC.SA 4.0) (http://creativecommons.org/licences/by-nc-sa/4.0/deed.es). Articles can be shared, copied, distributed, modified, altered, transformed into a derivative work, executed and publicly communicated, provided a) the authors and the original publication (Journal, Publisher and URL) are mentioned, b) they are not used for commercial purposes, c) the same terms of the license are maintained.
In the event that the manuscript is approved for its next publication, the authors retain the copyright and will assign to the journal the rights of publication, edition, reproduction, distribution, exhibition and communication at a national and international level in the different databases. data, repositories and portals.
It is hereby stated that the mentioned manuscript has not been published and that it is not being printed in any other national or foreign journal.
The authors hereby accept the necessary modifications, suggested by the reviewers, in order to adapt the manuscript to the style and publication rules of this Journal.

















