
Fibrous dysplasia of the lumbar spine in a middle-aged woman. Case presentation
Abstract
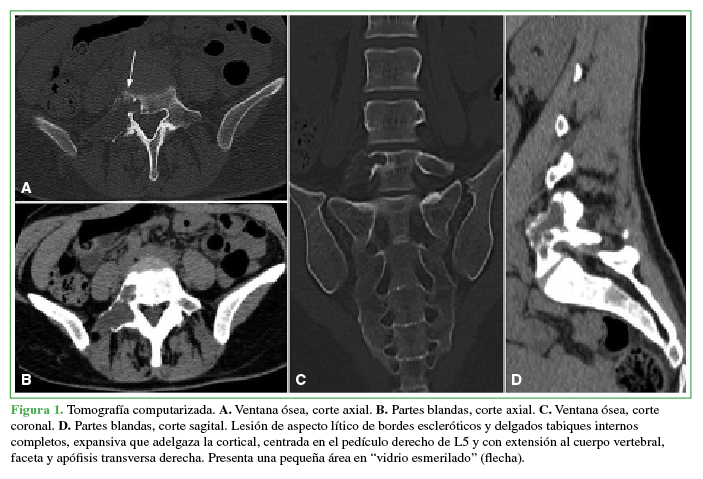
Abstract Fibrous dysplasia (FD) is a benign skeletal disorder characterized by abnormal development of fibrous tissue in a whorled pattern and containing trabeculae of immature non-lamellar bone. FD has two forms of clinical presentations: monostotic and polyostotic. Spinal involvement is seen mostly in the polyostotic form and is very unusual in the monostotic form. We present a 46-year-old woman that complained of right low back pain with a 2-month evolution. The definitive diagnosis was FD of the lumbar spine. Imaging testing revealed a lytic-cystic monostotic lesion with internal septa located in the posterior arch of the fifth lumbar vertebra, suggestive of Aneurysmal Bone Cyst (ABC). However, the anatomical pathology revealed FD as the final diagnosis. Conservative treatment was undertaken due to minimal symptoms and the absence of complications. Although monostotic FD of lumbar spine is rare, it should be taken into account among the differential diagnoses of a single osteolytic lesion. However, histopathology testing cannot rule out the coexistence of FB and ABC or a setting of FB secondary to an ABC.Downloads
References
Rodallec M, Feydy A, Larousserie F, Anract P, Campagna R, Babinet A, et al. Diagnostic imaging of solitary tumors of the spine: what to do and say. Radiographics 2008;28(4):1019-41. https://dx.doi.org/10.1148/rg.284075156
Murphey M, Andrews C, Flemming D, Temple T, Smith S, Smirniotopoulos J. From the archives of the AFIP. Primary tumors of the spine: radiologic pathologic correlation. Radiographics 1996;16(5):1131-58. https://dx.doi.org/10.1148/radiographics.16.5.8888395
Miller T. Bone tumors and tumor-like conditions: analysis with conventional radiography. Radiology 2008;246(3):662-74. https://doi.org/10.1148/radiol.2463061038
Remotti F, Feldman F. Nonneoplastic lesions that simulate primary tumors of bone. Arch Pathol Lab Med 2012;136(7):772-88. https://doi.org/10.5858/arpa.2011-0557-RA
Chow LTC, Griffith J, Chow WH, Kumta SM. Monostotic fibrous dysplasia of the spine: report of a case involving the lumbar transverse process and review of the literature. Arch Orthop Trauma Surg 2000;120(7):460-4. https://doi.org/10.1007/pl00013774
Fitzpatrick K, Taljanovic M, Speer D, Graham A, Jacobson J, Barnes J, et al. Imaging findings of fibrous dysplasia with histopathologic and intraoperative correlation. AJR Am J Roentgenol 2004;182(6):1389-98. https://doi.org/10.2214/ajr.182.6.1821389
Park H, Yang S, Sheppard W, Hegde V, Zoller S, Nelson S, et al. Current management of aneurysmal bone cysts. Curr Rev Musculoskelet Med 2016;9(4):435-44. https://doi.org/10.1007/s12178-016-9371-6
Munday T, Jobnson M, Whayes C, Thompson E, Smokei W. Musculoskeletal causes of spinal axis compromise: beyond the usual suspects. Radiographics 1994;14(6):1225-45. https://doi.org/10.1148/radiographics.14.6.7855338
Buraczewski J, Dabska M. Pathogenesis of aneurysmal bone cyst. Relationship between the aneurysmal bone cyst and fibrous dysplasia of bone. Cancer 1971;28(3):597-604. https://doi.org/10.1002/1097-0142(197109)28:3<597::aid-cncr2820280311>3.0.co;2-i
Kransdorf M, Sweet D. Aneurysmal bone cyst: concept, controversy, clinical presentation, and imaging. AJR Am J Roentgenol 1995;164(3):573-80. https://doi.org/10.2214/ajr.164.3.7863874
Lee JW, Kim JH, Han SH, Kang HI. Fibrous dysplasia with aneurysmal bone cyst presenting as painful solitary skull lesion. J Korean Neurosurg Soc 2010;48(6):551-4. https://doi.org/10.3340/jkns.2010.48.6.551
Martinez V, Sissons HA. Aneurysmal bone cyst. A review of 123 cases including primary lesions and those secondary to other bone pathology. Cancer 1988;61(11):2291-2304. https://doi.org/10.1002/1097-0142(19880601)61:11<2291::aid-cncr2820611125>3.0.co;2-v
Asazuma T, Sato M, Masuoka K, Yasuoka H, Tsuji T, Aida S. Monostotic fibrous dysplasia of the lumbar spine. Case report and review of the literature. J Spinal Disord Tech 2005;18(6):535-8. https://doi.org/10.1097/01.bsd.0000127703.75711.e7
Manuscript acceptance by the Journal implies the simultaneous non-submission to any other journal or publishing house. The RAAOT is under the Licencia Creative Commnos Atribución-NoComercial-Compartir Obras Derivadas Igual 4.0 Internacional (CC-BY-NC.SA 4.0) (http://creativecommons.org/licences/by-nc-sa/4.0/deed.es). Articles can be shared, copied, distributed, modified, altered, transformed into a derivative work, executed and publicly communicated, provided a) the authors and the original publication (Journal, Publisher and URL) are mentioned, b) they are not used for commercial purposes, c) the same terms of the license are maintained.
In the event that the manuscript is approved for its next publication, the authors retain the copyright and will assign to the journal the rights of publication, edition, reproduction, distribution, exhibition and communication at a national and international level in the different databases. data, repositories and portals.
It is hereby stated that the mentioned manuscript has not been published and that it is not being printed in any other national or foreign journal.
The authors hereby accept the necessary modifications, suggested by the reviewers, in order to adapt the manuscript to the style and publication rules of this Journal.

















